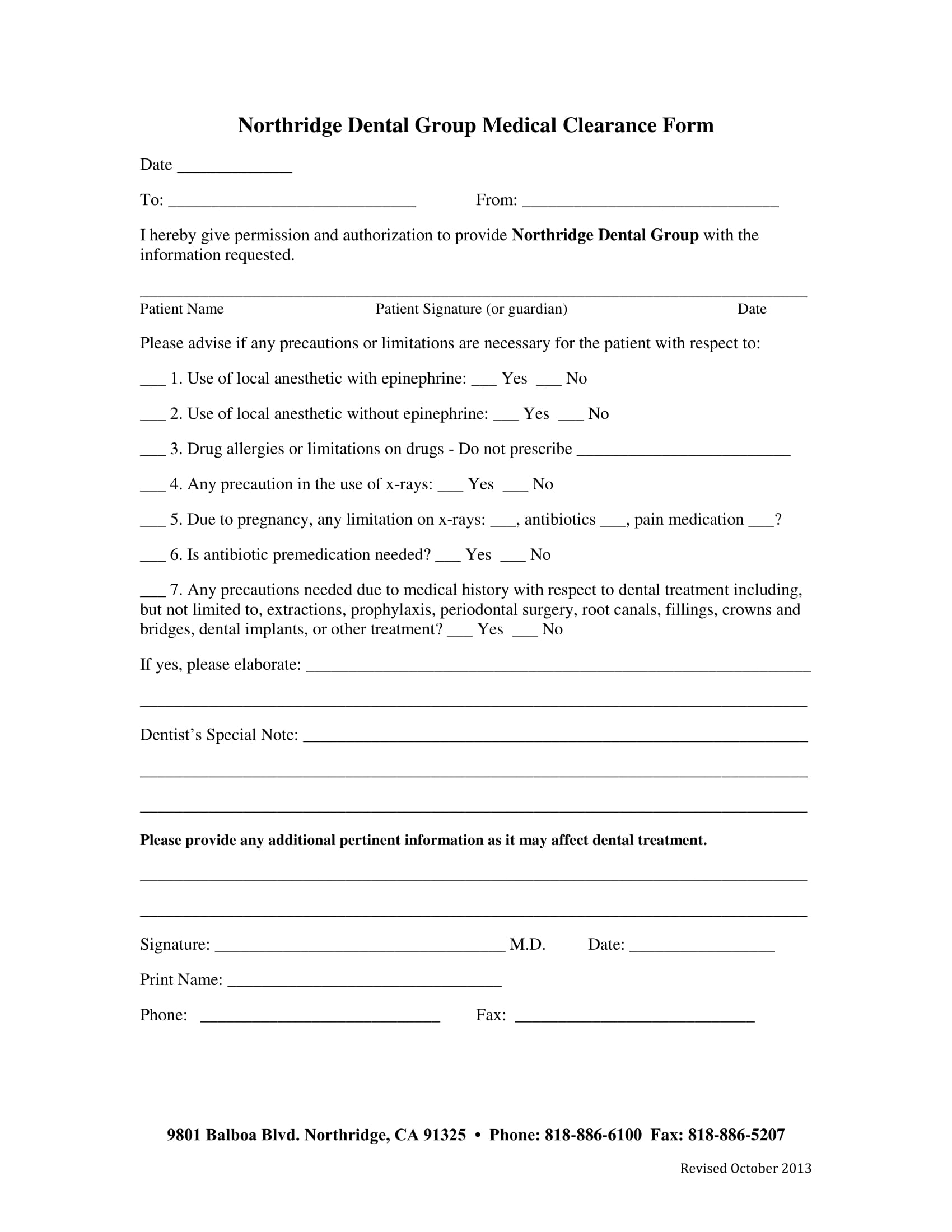
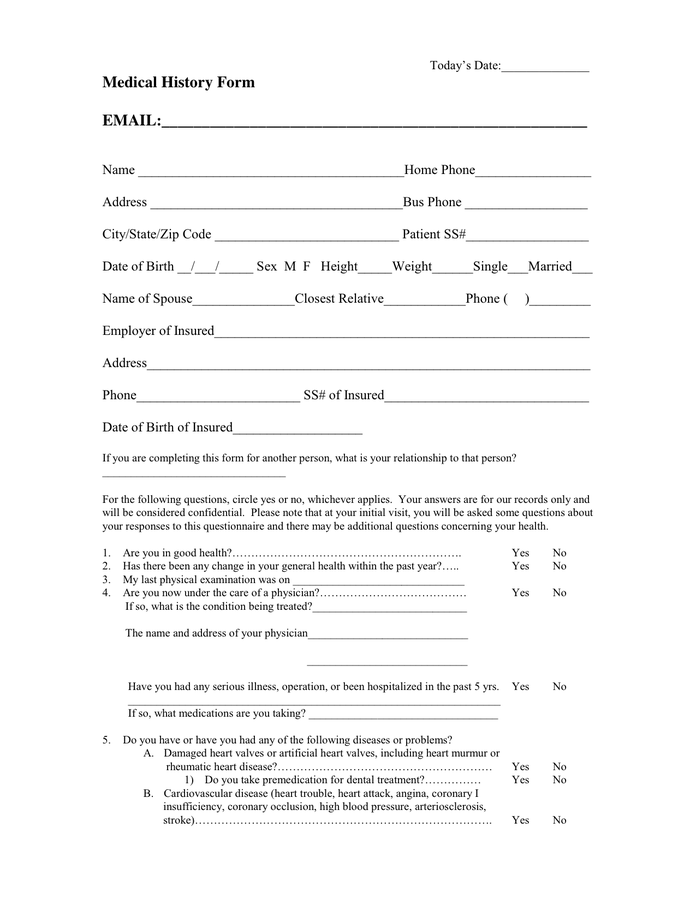
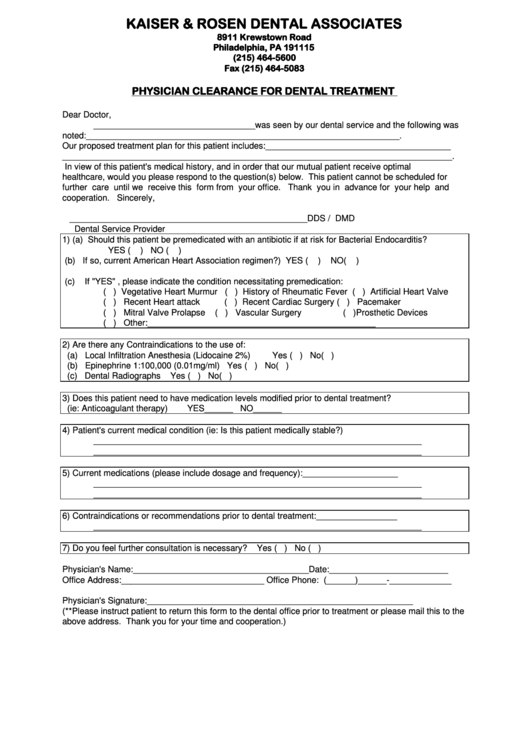
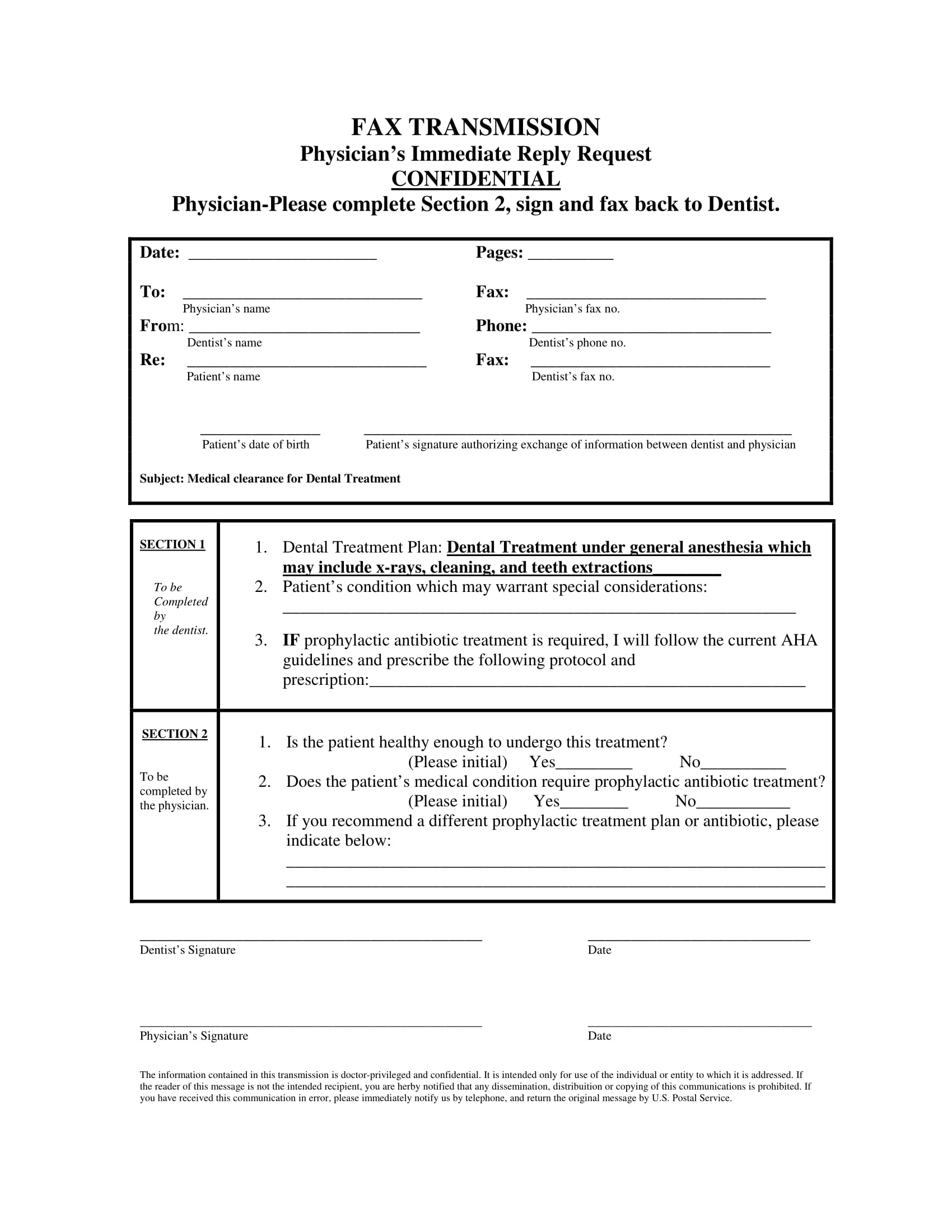
Medical Clearance Form For Dental Treatment - Medical clearance for dental treatment patient’s name:_________________________. A form for patients to fill out and sign before dental treatment, indicating their medical. We appreciate your assistance in. Our mutual patient is scheduled for dental treatment.
A form for patients to fill out and sign before dental treatment, indicating their medical. Our mutual patient is scheduled for dental treatment. Medical clearance for dental treatment patient’s name:_________________________. We appreciate your assistance in.
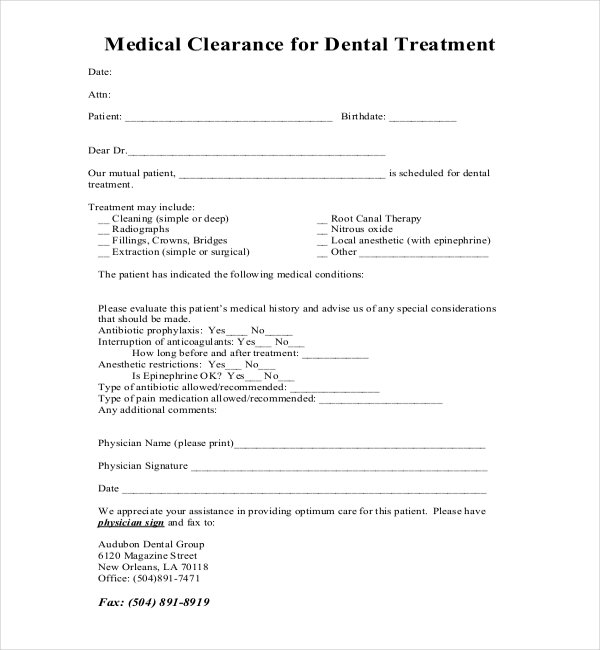
Our mutual patient is scheduled for dental treatment. Medical clearance for dental treatment patient’s name:_________________________. A form for patients to fill out and sign before dental treatment, indicating their medical. We appreciate your assistance in.
Printable Medical Clearance Form For Dental Treatment Printable Forms
A form for patients to fill out and sign before dental treatment, indicating their medical. Medical clearance for dental treatment patient’s name:_________________________. Our mutual patient is scheduled for dental treatment. We appreciate your assistance in.

Printable medical clearance form for dental treatment Fill out & sign
Our mutual patient is scheduled for dental treatment. We appreciate your assistance in. Medical clearance for dental treatment patient’s name:_________________________. A form for patients to fill out and sign before dental treatment, indicating their medical.
Dental Medical Clearance Form Printable Printable Word Searches
A form for patients to fill out and sign before dental treatment, indicating their medical. Medical clearance for dental treatment patient’s name:_________________________. We appreciate your assistance in. Our mutual patient is scheduled for dental treatment.
Printable Medical Clearance Form For Dental Treatment Printable Forms
A form for patients to fill out and sign before dental treatment, indicating their medical. We appreciate your assistance in. Medical clearance for dental treatment patient’s name:_________________________. Our mutual patient is scheduled for dental treatment.
27+ Sample Medical Clearance Forms Sample Forms
A form for patients to fill out and sign before dental treatment, indicating their medical. We appreciate your assistance in. Medical clearance for dental treatment patient’s name:_________________________. Our mutual patient is scheduled for dental treatment.

Printable Medical Clearance Form For Dental Treatment
A form for patients to fill out and sign before dental treatment, indicating their medical. Our mutual patient is scheduled for dental treatment. Medical clearance for dental treatment patient’s name:_________________________. We appreciate your assistance in.

Printable Dental Clearance Form Printable Computer Tools
Our mutual patient is scheduled for dental treatment. Medical clearance for dental treatment patient’s name:_________________________. A form for patients to fill out and sign before dental treatment, indicating their medical. We appreciate your assistance in.
Medical Clearance Form For Dental Treatment templates free printable
We appreciate your assistance in. Medical clearance for dental treatment patient’s name:_________________________. A form for patients to fill out and sign before dental treatment, indicating their medical. Our mutual patient is scheduled for dental treatment.
Physician Clearance For Dental Treatment Form printable pdf download
A form for patients to fill out and sign before dental treatment, indicating their medical. Our mutual patient is scheduled for dental treatment. We appreciate your assistance in. Medical clearance for dental treatment patient’s name:_________________________.
Printable Medical Clearance Form For Dental Treatment Printable Word
Our mutual patient is scheduled for dental treatment. A form for patients to fill out and sign before dental treatment, indicating their medical. We appreciate your assistance in. Medical clearance for dental treatment patient’s name:_________________________.
A Form For Patients To Fill Out And Sign Before Dental Treatment, Indicating Their Medical.
Our mutual patient is scheduled for dental treatment. Medical clearance for dental treatment patient’s name:_________________________. We appreciate your assistance in.