Sleep Study Order Form - Physicians order for home sleep test patient name:_____ ssn:_____. If a sleep study is. I certify that above home sleep test is medically indicated and is reasonable and necessary with.
Physicians order for home sleep test patient name:_____ ssn:_____. If a sleep study is. I certify that above home sleep test is medically indicated and is reasonable and necessary with.
Physicians order for home sleep test patient name:_____ ssn:_____. If a sleep study is. I certify that above home sleep test is medically indicated and is reasonable and necessary with.

Fillable Online INHOME DIAGNOSTIC SLEEP STUDY REQUEST FORM Fax Email
Physicians order for home sleep test patient name:_____ ssn:_____. If a sleep study is. I certify that above home sleep test is medically indicated and is reasonable and necessary with.

Sleep Study Order (FSL30). Doc Template pdfFiller
I certify that above home sleep test is medically indicated and is reasonable and necessary with. If a sleep study is. Physicians order for home sleep test patient name:_____ ssn:_____.
When To Order A Sleep Study IntraBalance
I certify that above home sleep test is medically indicated and is reasonable and necessary with. Physicians order for home sleep test patient name:_____ ssn:_____. If a sleep study is.
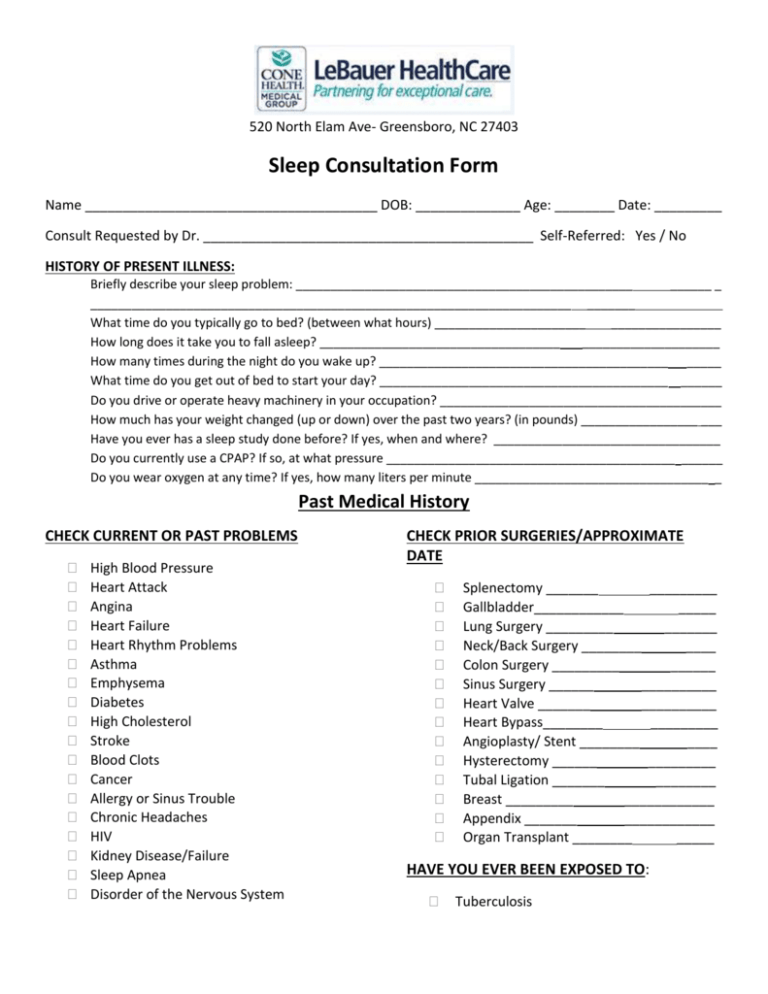
Sleep Consultation Form
I certify that above home sleep test is medically indicated and is reasonable and necessary with. Physicians order for home sleep test patient name:_____ ssn:_____. If a sleep study is.

Fillable Online Sleep Study Order Form Fill Online, Printable
If a sleep study is. I certify that above home sleep test is medically indicated and is reasonable and necessary with. Physicians order for home sleep test patient name:_____ ssn:_____.

Fillable Online SLEEP STUDY ORDER FORM HOME Sleep Centers of Texas
I certify that above home sleep test is medically indicated and is reasonable and necessary with. If a sleep study is. Physicians order for home sleep test patient name:_____ ssn:_____.
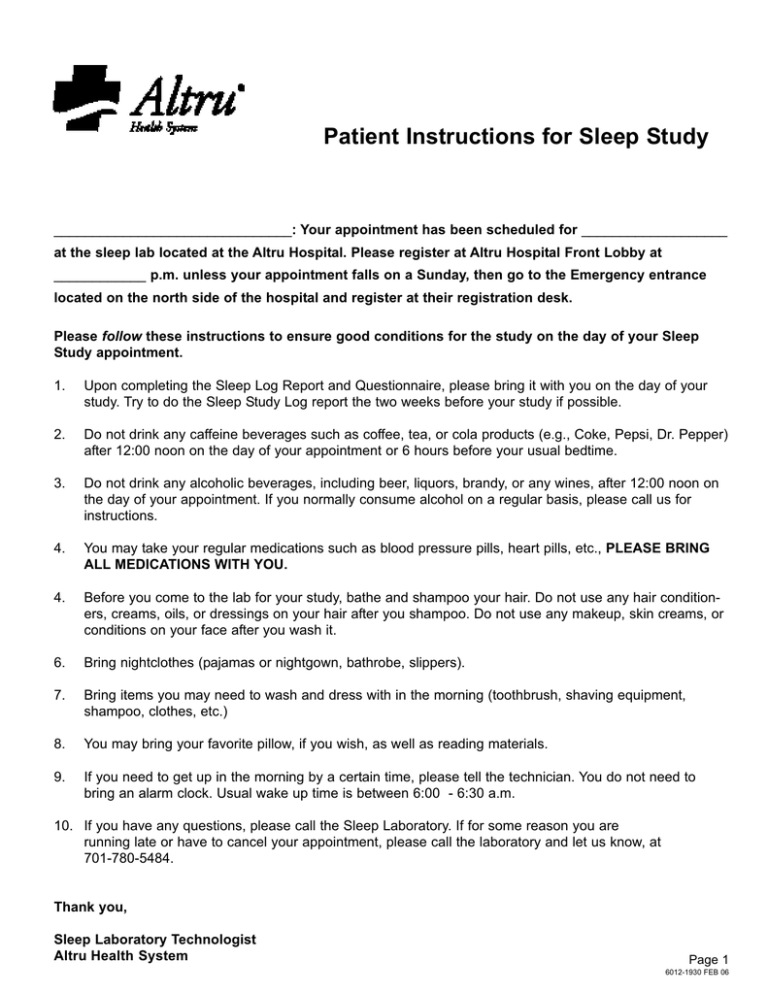
Patient Instructions for Sleep Study
I certify that above home sleep test is medically indicated and is reasonable and necessary with. Physicians order for home sleep test patient name:_____ ssn:_____. If a sleep study is.

Sleep Study What It Is and What to Expect
I certify that above home sleep test is medically indicated and is reasonable and necessary with. If a sleep study is. Physicians order for home sleep test patient name:_____ ssn:_____.

Sleep Study PDF
I certify that above home sleep test is medically indicated and is reasonable and necessary with. Physicians order for home sleep test patient name:_____ ssn:_____. If a sleep study is.

Sleep Study Instructions PDF
Physicians order for home sleep test patient name:_____ ssn:_____. I certify that above home sleep test is medically indicated and is reasonable and necessary with. If a sleep study is.
If A Sleep Study Is.
I certify that above home sleep test is medically indicated and is reasonable and necessary with. Physicians order for home sleep test patient name:_____ ssn:_____.